If you are dealing with a nagging, sharp ache on the outside of your elbow, your first instinct might be confusion—especially if you haven’t picked up a tennis racket in years.
Despite its famous nickname, Tennis Elbow—medically termed Lateral Epicondylalgia (LE)—is rarely an injury exclusive to athletes. In fact, it is estimated that only about 10% of individuals affected by this disorder actually play tennis (Johns & Shridhar, 2020). Instead, it is highly prevalent among office workers, full-time keyboard users, and digital professionals (Bretschneider et al., 2021; Mallen et al., 2011).
If your day-to-day involves hours of typing, clicking, and desk work, here is a breakdown of why your forearm tendons are irritated and what you can do about it.

The Pathophysiology: What is Actually Happening?
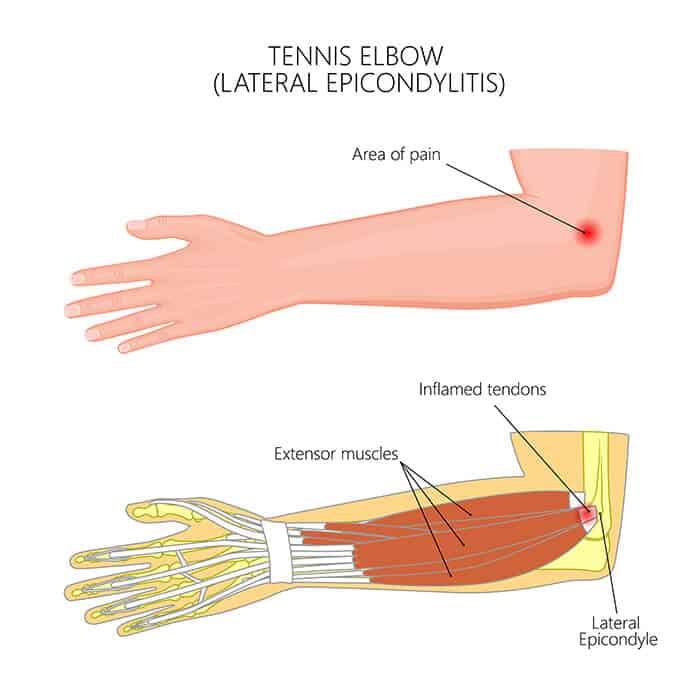
To understand why office work triggers this pain, we have to look at the anatomy of your forearm. The muscles that lift your wrist and fingers up (extension) converge into a single, shared anchor point on the outside of your elbow called the common extensor tendon (Buchanan, 0). The primary culprit in lateral epicondylalgia is a specific muscle called the Extensor Carpi Radialis Brevis (ECRB) (Buchanan, 0; Karabinov & Georgiev, 2022).
While older medical texts classified tennis elbow as a purely inflammatory “tendonitis,” modern tissue biopsies reveal a different story. The condition is actually a tendinosis—a degenerative process characterized by microscopic structural failure, unstructured collagen, and micro-tears rather than traditional inflammatory cells (Buchanan, 0; Vaquero-Picado et al., 2016). When a tendon is repeatedly loaded beyond its physiological capacity, the body struggles to repair it correctly, leading to a weak, disorganized tendon structure that registers as persistent pain.
Why Typing and Mouse Work Overload Your Elbow
It might seem strange that typing—an activity that feels relatively effortless—can cause structural breakdown. The problem lies in sustained isometric contraction and micro-repetitive strain.
Hovering fingers – Constant Isometric Tension on ECRB Muscle – Reduced Local Blood Flow & Cumulative Micro-trauma – Tendon Tissue Breakdown (Tendinosis)
- The “Hovering” Finger Strain: When you type, your fingers don’t just collapse onto the keys; your wrist extensors must contract constantly to keep your hands raised and positioned over the keyboard. This prolonged, low-level contraction starves the tendon of optimal blood flow (Karabinov & Georgiev, 2022).
- The Mechanical Disadvantage of the Mouse: Gripping a computer mouse requires a combination of continuous forearm pronation (turning the palm down) and static wrist extension. Studies indicate that computer use of more than 20 hours per week significantly amplifies the risk of developing lateral epicondylalgia, with risks compounding over years of employment (Mallen et al., 2011).
- The “Death Grip”: Gripping a mouse too tightly or forcefully pinching modern thin devices places an eccentric overload on the ECRB tendon insertion point (Buchanan, 0; Johns & Shridhar, 2020). Over an eight-hour workday, these micro-strains accumulate into macro-irritation.
Clinical Implications for Recovery
If you are treating office-related tennis elbow, the evidence emphasizes that standard rest or passive treatments alone rarely solve the long-term issue (Waugh et al., 2004). Because computer use is associated with a more persistent long-term prognosis, recovery must focus directly on modifying your daily workstation habits and progressively rebuilding tendon resilience (Waugh et al., 2004).
Ergonomic Checklist for Forearm Relief
| Ergonomic Variable | Sub-optimal Setup (High Strain) | Optimal Setup (Low Strain) |
| Wrist Position | Extended upward or tilted to the side | Neutral, straight alignment parallel to desk |
| Mouse Design | Standard flat mouse (forces full pronation) | Vertical mouse (places forearm in neutral “handshake” posture) |
| Keyboard Height | Too high, forcing elbows to bend past 90° | Elbows resting comfortably at a 90° to 100° angle |
The Physio Perspective
Corticosteroid injections may provide rapid, short-term relief, but clinical evidence shows they are associated with high rates of long-term recurrence (Mallen et al., 2011; Vaquero-Picado et al., 2016). The gold standard for true recovery is progressive, targeted exercise loading—such as eccentric and slow isometric loading—which actively stimulates the tendon to rebuild organized, strong collagen fibers (Vaquero-Picado et al., 2016).
If your desk job is making your elbow scream, resting it over the weekend isn’t a permanent fix. Modifying your workspace ergonomics and structurally strengthening the forearm extensors are the most reliable ways to get back to pain-free productivity.
References
Bretschneider, S. F., Los, F. S., Eygendaal, D., Kuijer, P. P. F. M., & van der Molen, H. F. (2021). Work‐relatedness of lateral epicondylitis: Systematic review including meta-analysis and GRADE work‐relatedness of lateral epicondylitis. American Journal of Industrial Medicine, 65(1), 41–50. https://doi.org/10.1002/ajim.23303
Buchanan, B. K. (n.d.). Lateral Epicondylitis (Tennis Elbow). StatPearls. https://doi.org/NBK431092
Johns, N., & Shridhar, V. (2020). Lateral epicondylitis: Current concepts. Australian Journal of General Practice, 49(11), 707–709. https://doi.org/10.31128/ajgp-07-20-5519
Karabinov, V., & Georgiev, G. P. (2022). Lateral epicondylitis: New trends and challenges in treatment. World Journal of Orthopedics, 13(4), 354–364. https://doi.org/10.5312/wjo.v13.i4.354
Mallen, C., Chesterton, & Hay. (2011). Management of tennis elbow. Open Access Journal of Sports Medicine, 53. https://doi.org/10.2147/oajsm.s10310
Vaquero-Picado, A., Barco, R., & Antuña, S. A. (2016). Lateral epicondylitis of the elbow. EFORT Open Reviews, 1(11), 391–397. https://doi.org/10.1302/2058-5241.1.000049
Waugh, J. E., Jaglal, S. B., & Davis, A. M. (2004). Computer Use Associated With Poor Long-Term Prognosis of Conservatively Managed Lateral Epicondylalgia. Journal of Orthopaedic & Sports Physical Therapy, 34(12), 770–780. https://doi.org/10.2519/jospt.2004.34.12.770