If you have ever suffered from a severe, throbbing headache that leaves you reaching for a dark room, your first thought is probably: “It’s another migraine.”
What many headache sufferers do not realize is that the true culprit might not be in their brain at all—it could be structural stiffness in the upper cervical joints of the neck. This condition is known as a cervicogenic headache (CGH), a secondary headache that stems directly from musculoskeletal dysfunction in the top three joints of your spine (Hall et al., 2008). Because the pain signals mimic primary headache disorders so perfectly, an estimated 50% of these cases are misdiagnosed (Anarte-Lazo et al., 2021).

How Stiff Neck Joints Impersonate a Migraine
The reason a neck issue can feel like a massive head explosion comes down to a structural “wiring crossover” in your nervous system.
Deep inside the upper spinal cord sits the trigeminocervical nucleus. This area acts as a major neurological junction box where sensory nerve fibers from your upper three neck joints ($C1$, $C2$, and $C3$) converge and overlap with the trigeminal nerve—the primary nerve responsible for sensation in your face and head (Chaibi & Russell, 2012).
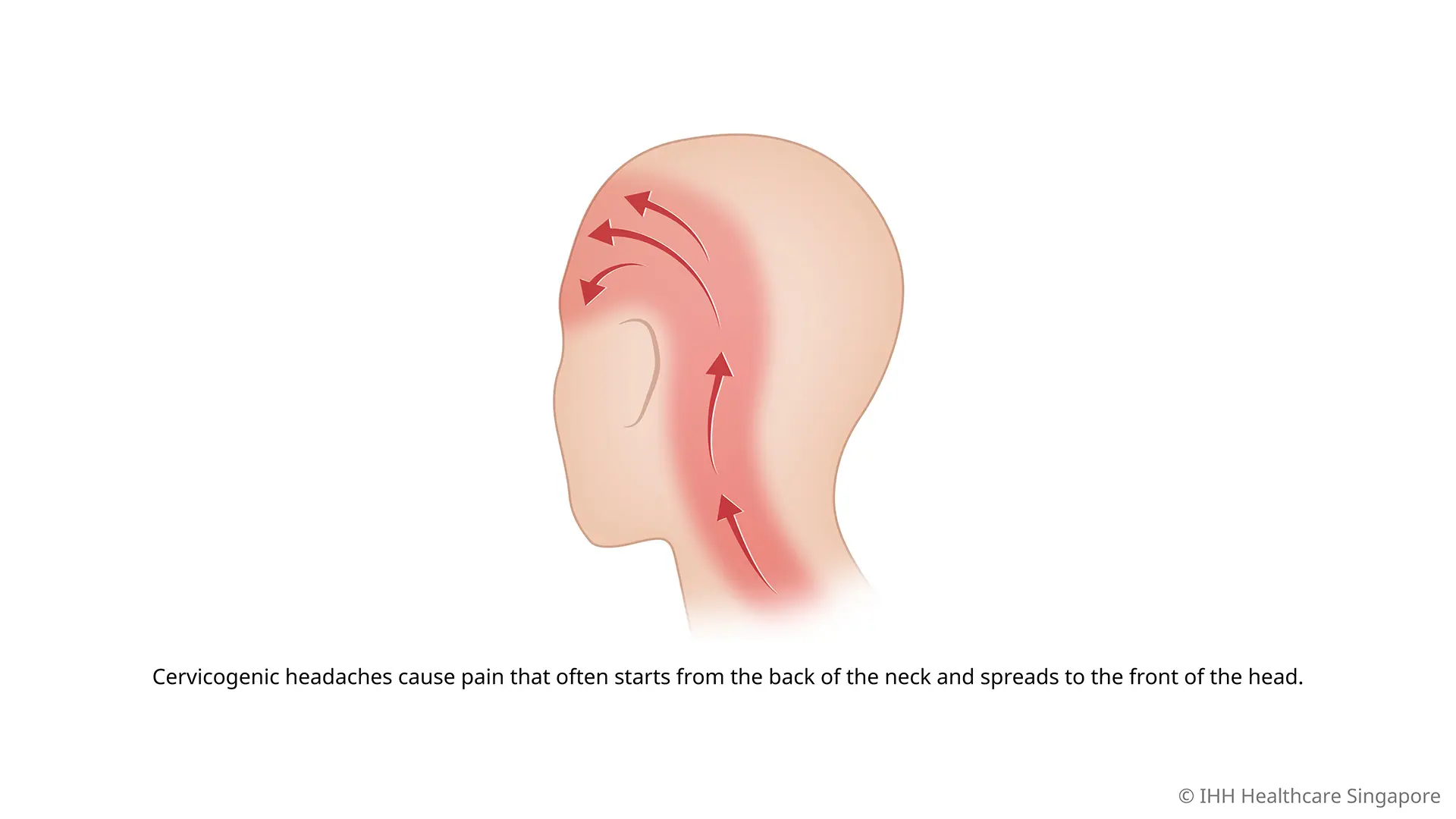
When poor posture, an old whiplash injury, or prolonged desk work causes the joints at the base of your skull to become stiff, locked, or inflamed, they fire off constant, low-grade distress signals. Because of this neurological convergence, your brain gets confused. It processes the pain signals coming from your stiff upper neck joints and interprets them as pain in your temple, forehead, or behind your eye (Al Khalili).
This crossover is so profound that a cervicogenic headache can even cause secondary “migraine-like” symptoms, including:
- Nausea or an upset stomach
- Sensitivity to light (photophobia) and sound
- Dizziness or blurred vision on one side (Chaibi & Russell, 2012).
The Tell-Tale Differences: Migraine vs. Cervicogenic
While they share a symptom pool, a physical assessment by a physiotherapist can quickly separate the two. A key indicator of a cervicogenic headache is that the pain is strictly unilateral (staying on one side of the head without shifting sides) and is directly triggered or worsened by specific neck movements, awkward sustained head positions, or external pressure applied to the base of the skull (Al Khalili). Furthermore, traditional migraine medications like triptans or ergotamines typically provide little to no relief for a neck-driven headache (Hall et al., 2008).
How Physiotherapy Clears the Pain
Because cervicogenic headaches are structural, they respond exceptionally well to targeted, hands-on physical therapy. Rather than simply masking the pain with medication, a physiotherapist works to resolve the underlying mechanical dysfunction using a multi-step approach:
- Targeted Joint Mobilization: Using precise, gentle manual therapy pressures, your physio can restore normal gliding motion to the stiff $C1$-$C3$ spinal segments. Restoring this joint mobility immediately dials down the hyperactive pain signaling to the trigeminocervical nucleus (Hall et al., 2008).
- Myofascial Trigger Point Therapy: Chronic joint stiffness causes the surrounding muscles—especially the suboccipitals and the sternocleidomastoid—to go into protective, painful spasms. Releasing these active trigger points significantly reduces both neck strain and referred head pain intensity (Bodes-Pardo et al., 2013).
- Deep Flexor Retraining: Research demonstrates that people with cervicogenic headaches frequently exhibit weakness in their deep neck stabilizing muscles (Anarte-Lazo et al., 2021). Your physio will guide you through progressive endurance exercises (like the craniocervical flexion test protocol) to build the deep muscle support needed to protect your neck from recurring stiffness (Bodes-Pardo et al., 2013).
If you are tired of managing recurring “migraines” with dark rooms and medication, the solution might be sitting just beneath the base of your skull. A comprehensive upper cervical assessment can determine if a stiff neck is driving your head pain, providing a clear, evidence-based pathway to lasting relief.
References
Al Khalili, Y. (2023). Cervicogenic headache. StatPearls. StatPearls Publishing.
Anarte-Lazo, E., Carvalho, G. F., Schwarz, A., Luedtke, K., & Falla, D. (2021). Differentiating migraine, cervicogenic headache and asymptomatic individuals based on physical examination findings: a systematic review and meta-analysis. BMC Musculoskeletal Disorders, 22(1), 755. https://doi.org/10.1186/s12891-021-04595-w
Bodes-Pardo, G., Pecos-Martín, D., Gallego-Izquierdo, T., Salom-Moreno, J., Fernández-de-las-Peñas, C., & Ortega-Santiago, R. (2013). Manual treatment for cervicogenic headache and active trigger point in the sternocleidomastoid muscle: a pilot randomized clinical trial. Journal of Manipulative and Physiological Therapeutics, 36(7), 403-411. https://doi.org/10.1016/j.jmpt.2013.05.022
Chaibi, A., & Russell, M. B. (2012). Manual therapies for cervicogenic headache: a systematic review. The Journal of Headache and Pain, 13(5), 351-359. https://doi.org/10.1007/s10194-012-0436-7
Hall, T., Briffa, K., & Hopper, D. (2008). Clinical evaluation of cervicogenic headache: a clinical perspective. Journal of Manual & Manipulative Therapy, 16(2), 73-80. https://doi.org/10.1179/106698108790818422