If you are feeling a sharp twinge or a persistent, dull ache on the inner side of your elbow, you are not alone. While commonly dubbed “Golfer’s Elbow,” medial epicondylitis is far from a problem exclusive to the fairway.
In reality, more than 90% of cases occur in non-athletes (Kiel, n.d.). It frequently targets individuals involved in labor-intensive occupations or activities that require repetitive gripping, heavy lifting, or forceful forearm rotation (Kiel, n.d.; Tahir, n.d.).
Whether your pain triggers during a golf swing, while carrying heavy tools, or simply when twisting open a jar, understanding the underlying biomechanics is the secret to a lasting recovery.

What is Golfer’s Elbow? (Hint: It’s Not Inflammation)
For years, the medical community labeled this condition an “-itis,” implying an acute inflammatory problem. Modern sports medicine tells a different story: medial epicondylitis is actually a degenerative tendinosis (Kiel, n.d.).
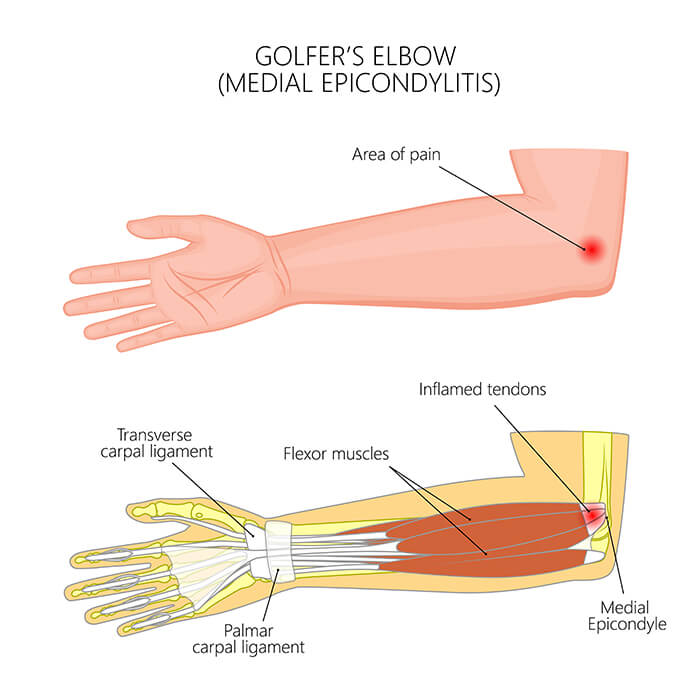
The inner prominence of your elbow (the medial epicondyle) serves as the anchor point for the common flexor tendon (Tahir, n.d.). This single tendon fuses together the primary muscles responsible for flexing your wrist and fingers and pronating (turning down) your forearm (Kiel, n.d.).
When these muscles are subjected to chronic, repetitive overload—particularly during forceful eccentric loading (when the muscle lengthens under tension)—it creates microscopic structural microtears in the tendon (Kiel, n.d.). Without structural remodeling, the tendon loses its organized architectural matrix, resulting in persistent discomfort and weakness (Tahir, n.d.).
The Core Fix: A Step-by-Step Loading Progression
Tendon tissue adapts beautifully to mechanical loading. Progressive resistance exercise upregulates collagen synthesis, effectively rebuilding the tendon’s internal structure from the inside out (Ellenbecker, 2013).
A structured, evidence-based physical therapy framework shifts your recovery from passive rest to active capacity building (Marotta, 2026):
1. Protected Function & Load Management: Phase 1.
Temporarily minimize or modify the activities that provoke sharp pain, such as heavy lifting or sustained gripping (Ellenbecker, 2013). The goal is to avoid total immobilization—which causes muscle atrophy—while protecting the tendon from excessive valgus stress (Kiel, n.d.; Ellenbecker, 2013).
2. Targeted Isometric Holds: Phase 2.
Begin introducing low-level static muscle contractions. Sit with your forearm supported, palm facing up, and apply gentle resistance with your opposite hand. Hold your wrist completely still against resistance for 30–45 seconds. Isometrics help build baseline load tolerance and provide a natural analgesic (pain-relieving) effect.
3. Controlled Eccentric Strengthening: Phase 3.
Once isometrics are comfortable, focus on the eccentric (lengthening) phase (Marotta, 2026). Use your uninjured hand to lift a light dumbbell into a flexed wrist position. Then, using only the injured arm, slowly lower the weight down over a controlled 5-second count (Tyler, 2014). Research demonstrates that isolated eccentric training significantly improves pain and grip strength (Yoon et al., 2021; Tyler, 2014).
4. Dynamic Rotational Stability: Phase 4.
Gradually integrate active forearm pronation and supination movements against light resistance (Marotta, 2026). This re-trains the pronator teres muscle to withstand torsional forces, ensuring full functional recovery for sport or occupational demands (Kiel, n.d.; Marotta, 2026).
Optimizing Your Upper Limb Biomechanics
Treating the elbow in isolation is a temporary band-aid. The elbow is a mechanical bridge trapped between your shoulder and your wrist. If you suffer from limited shoulder mobility or poor scapular stability, your nervous system will naturally force the forearm muscles to compensate, leading to overloading at the medial epicondyle.
The Multidisciplinary Link: Clinical assessments indicate that up to 60% of medial epicondylitis cases present with concomitant ulnar nerve irritation or dynamic instability (Ryskalin, 2026). This occurs because the ulnar nerve sits directly behind the medial epicondyle (Ryskalin, 2026). Addressing whole-arm mechanics and tracking patterns is crucial to keeping the nerve and the tendon moving smoothly without compression (Ryskalin, 2026).
If you are tired of dealing with nagging elbow pain and want a tailored biomechanical assessment to pinpoint exactly why your tendon is overloaded, let’s get you sorted.
References
- Ellenbecker, T. S. (2013). Current concepts in examination and treatment of elbow tendon injury. Ovid, 32(2), 1-15.Cited by: 64
- Kiel, J. (n.d.). Medial Epicondylitis (Golfer’s Elbow). StatPearls – NCBI Bookshelf.Cited by: 25
- Marotta, N. (2026). The role of kinematic and electromyographic analysis of the elbow in arm wrestlers. MDPI, 16(2), 713.Cited by: 3
- Ryskalin, L. (2026). Application of extracorporeal shockwave therapy in medial epicondylitis with concomitant ulnar nerve instability: A case series with long-term follow-up. Frontiers, 7, 1677404.
- Tahir, A. (n.d.). Medial Epicondylitis: A review of clinical presentation, diagnosis, and management in the United Kingdom. PMC, 12(3), 12931734.
- Tyler, T. F. (2014). Clinical outcomes of the addition of eccentrics for rehabilitation of previously failed treatments of golfers elbow. PMC, 9(3), 4060314.Cited by: 27
- Yoon, S. Y., Kim, Y. W., Shin, In S., Kang, S., Moon, H. I., & Lee, S. C. (2021). The beneficial effects of eccentric exercise in the management of lateral elbow tendinopathy: A systematic review and meta-analysis. Journal of Clinical Medicine, 10(17), 3968. https://doi.org/10.3390/jcm10173968Cited by: 87