If you are reading this while holding your arm perfectly still, terrified to move your shoulder even an inch, you are not alone. Acute subacromial bursitis—the painful inflammation of the fluid-filled sac (bursa) that cushions the bones and tendons in your shoulder—is famous for coming out of nowhere and hitting hard. One day you are fine, and the next, putting on a t-shirt or reaching for a cup feels like a sharp shock to your joint. When your bursa is this angry, your brain’s natural response is to freak out and freeze. But hitting the panic button won’t help. Instead, let’s look at the evidence-based, immediate steps you can take today to cool off that painful shoulder inflammation and start tracking back toward normal movement.

1. What Exactly Just Happened?
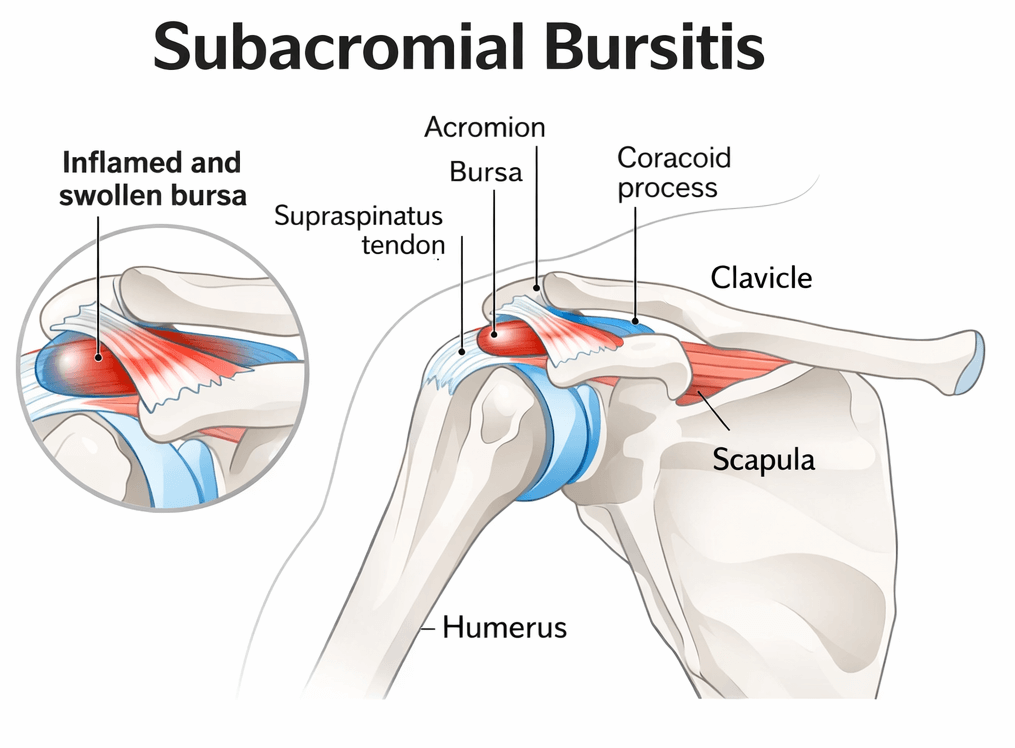
Deep inside your shoulder, directly underneath the bony tip of your shoulder blade (the acromion), sits your subacromial bursa. In a healthy joint, this small, fluid-filled pad acts like a frictionless pillow, preventing your rotator cuff tendons from scraping against bone during
overhead movements. However, if you suddenly overload the arm, tweak it awkwardly, or suffer from underlying postural imbalances, that bursa can get pinched and highly inflamed. Clinical definitions classify Subacromial Pain Syndrome (SAPS) as non-traumatic, regional shoulder pain that flares up intensely during arm elevation (Diercks et al., 2014; Heerspink, 2026). When the bursa swells, the space inside the joint shrinks, turning every basic movement into a painful pinch.
2. The Immediate “Calm Down” Blueprint
In the first 48 to 72 hours of an acute flare-up, your primary objective isn’t to build strength or stretch things out. Your only job is to reduce the chemical firestorm inside the joint. Here is your immediate management plan:
Step 1: Enforce Relative Rest (Not Total Immobilization)
Stop doing whatever triggered the pain—especially overhead lifting, reaching behind your back, or sleeping directly on that arm. However, do not put your arm in a sling or freeze it completely. Strict immobilization is highly discouraged by clinical guidelines as it increases the long-term risk of developing a frozen shoulder (Diercks et al., 2014). Move your arm gently within a completely pain-free zone.
Step 2: Cool Down the Tissue
Apply an ice pack wrapped in a damp towel to the tip of your shoulder for 15 to 20 minutes every few hours. This local cryotherapy constricts the blood vessels, dialing down active swelling and providing a natural numbing effect to the irritated nerve endings.
Step 3: Manage the Chemical Inflammation
Because acute bursitis is primarily an inflammatory issue, standard pain relievers may not cut it. Short-term use of oral non-steroidal anti-inflammatory drugs (NSAIDs) can significantly lower pain levels during the initial 1 to 2 weeks (Diercks et al., 2014).
Important Note: Always consult your pharmacist or general practitioner before beginning any new medication to ensure NSAIDs are safe for your stomach and cardiovascular health.
3. Gentle Movement: 2 Exercises for Day 1
Once the baseline, throbbing pain begins to ease slightly, you can introduce low-intensity, non-threatening movements. These exercises are designed to keep the joint lubricated without pinching the bursa. If you feel a sharp, catching pain, stop immediately.
1. The Pendulum Hang: 1-2 minutes, 3 times a day.
Lean forward and support your healthy arm on a sturdy table or kitchen counter. Let your painful arm hang straight down toward the floor like a ragdoll. Gently sway your body back and forth, letting the momentum naturally swing your relaxed arm in tiny, effortless circles. This creates a mild traction effect, gently widening the subacromial space to relieve pressure on the bursa.
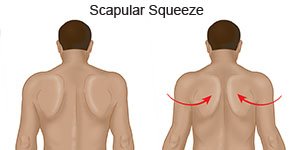
2. Gentle Shoulder Blade Squeezes: 10-15 repetitions, twice daily.
Sit or stand with tall, relaxed posture. Without moving your arm or raising your shoulders toward your ears, gently draw your shoulder blades back and together as if squeezing a pen between them. Hold for 5 seconds, then release. This activates your lower trapezius and rhomboids, pulling the acromion slightly backward and preventing it from compressing the bursa.
4. The Physiotherapy Path Forward
Once the acute flame is reduced to a flicker, true recovery begins. Research consistently highlights that structured, physiotherapist-led exercise programs yield vastly superior results for long-term shoulder function and pain reduction compared to generic advice sheets (Roddy et
al., 2020). Your physiotherapist will guide you through a phased rehab plan built around targeted movement:
| Phase | Main Focus | Typical Strategy |
| Phase 1: Acute | Inflammation Control | Cryotherapy, relative rest, pain-free active range of motion. |
| Phase 2: Sub-Acute | Rotator Cuff Coordination | Low-load isometric exercises to stabilize the humeral head. |
| Phase 3: Remodeling | Progressive Loading | Specific resistance band training to build long-term structural resilience (Zhu et al., 2021). |
When to Consider a Subacromial Corticosteroid Injection
If your pain is so severe that you cannot sleep, dress, or even begin gentle exercise therapy, you may be a candidate for a subacromial corticosteroid injection. Clinical trials prove that subacromial corticosteroid injections provide powerful, highly effective short-term pain relief within the first 6 to 8 weeks (Diercks et al., 2014). Think of an injection not as a permanent cure, but as a clinical window of opportunity. It quickly knocks out the inflammation so that you can actively engage in the progressive resistance training required to fix the underlying mechanical cause (Chang, 2026; Zhu et al., 2021).
Take a Deep Breath
An acute shoulder flare-up is incredibly frustrating, but your bursa will settle down. Prioritize resting it from overhead tasks, cool it down with ice, move it gently within a safe zone, and schedule an appointment with a physiotherapist to build a roadmap back to pain-free performance.
References
Chang, Y. C. (2026). Efficacy of a mobile health-supported home-based resistance exercise after ultrasound-guided corticosteroid injection in chronic subacromial bursitis: A randomized controlled trial. Journal of Clinical Medicine, 15(7), 2567.
Diercks, R., Bron, C., Dorrestijn, O., Meskers, C., Naber, R., de Ruiter, T., Willems, J., Winters, J., & van der Woude, H. J. (2014). Guideline for diagnosis and treatment of subacromial pain syndrome. Acta Orthopaedica, 85(3), 314-322. https://doi.org/10.3109/17453674.2014.920991
Heerspink, F. O. L. (2026). Update of guideline for diagnosis and treatment of subacromial pain syndrome: a multidisciplinary review by the Dutch Orthopedic Association Part 1: preventive measures, diagnostics, and non-surgical treatment of subacromial pain syndrome. ActaOrthopaedica, 97(1), 112-125.
Roddy, E., Ogollah, R. O., Oppong, R., Zwierska, I., Datta, P., Hall, A., Hay, E., Jackson, S., Jowett, S., Lewis, M., Shufflebotham, J., Stevenson, K., van der Windt, D. A., Young, J., & Foster, N. E. (2020). Optimising outcomes of exercise and corticosteroid injection in patients with subacromial pain (impingement) syndrome: a factorial randomised trial. British Journal of Sports Medicine, 55(5), 262-271. https://doi.org/10.1136/bjsports-2019-101268
Zhu, P., Liao, B., Wang, Z., Sun, Z., Wei, Y., & Cai, Y. (2021). Resistance band training after triamcinolone acetonide injection for subacromial bursitis: A randomized clinical trial. Journal of Rehabilitation Medicine, 53(5), jrm00140. https://doi.org/10.2340/16501977-2752