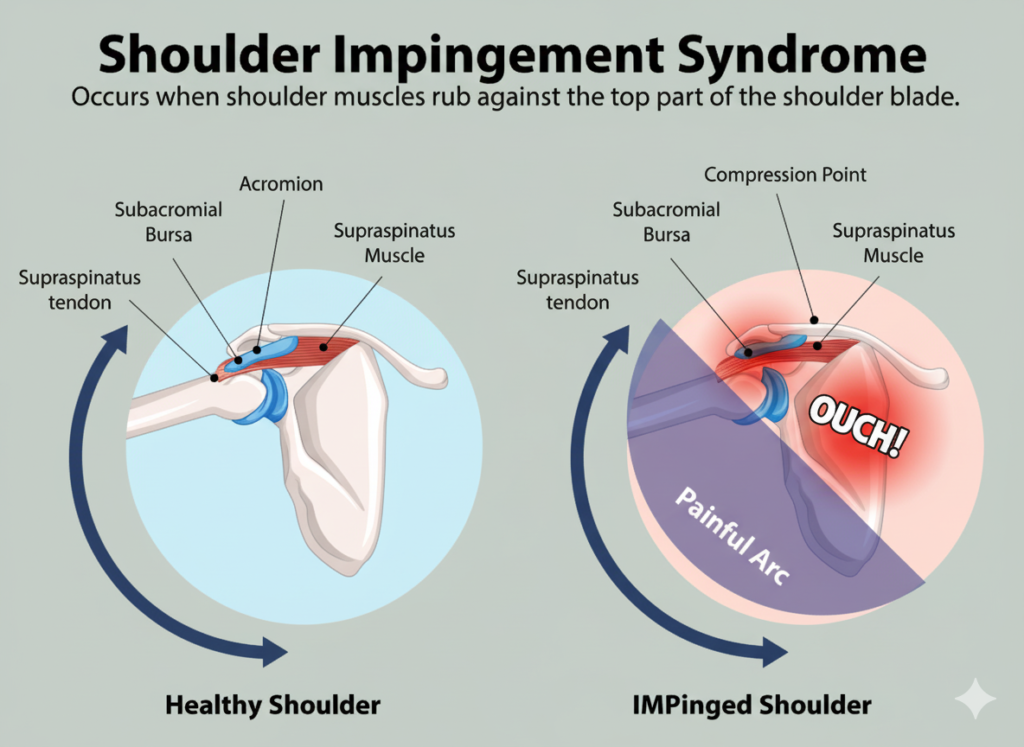
Shoulder impingement syndrome describes pain that occurs when structures in the subacromial space (usually the rotator cuff tendons and the subacromial bursa) are irritated and compressed during arm elevation. It’s one of the most common reasons people seek help for shoulder pain. Diagnosis is primarily clinical, based on history and examination. NCBI
Why it happens
Impingement can be grouped in two ways:
- External (subacromial) vs. internal: External involves compression beneath the acromion; internal occurs when the rotator cuff is pinched between the humeral head and glenoid rim (often in throwers). NCBI
- Primary vs. secondary: Primary relates to structural narrowing (e.g., a hooked acromion or soft-tissue swelling). Secondary arises from movement control issues such as rotator-cuff or scapular muscle weakness that let the humeral head migrate upward during elevation. NCBI
Who is at risk?
People who perform repetitive overhead activity (e.g., swimmers, throwers, painters, carpenters, hairdressers) are commonly affected. Incidence increases with age, and smoking, heavy load bearing, and certain antibiotics (fluoroquinolones) are additional risk factors. NCBI
Typical symptoms
- Pain when lifting the arm or lying on the sore side
- Night pain and sleep disturbance
- Gradual onset over weeks to months, often without a single injury
- Pain over the outer shoulder, sometimes spreading down the upper arm
Weakness or stiffness may be secondary to pain rather than true muscle failure. NCBI
How clinicians examine it
Your physio will compare both shoulders and check posture, range, strength, and scapular control. Common provocation tests include Hawkins, Neer, Jobe/Empty-Can, and a painful arc between ~70–120°. No single test is perfect, but a cluster of findings builds diagnostic confidence. NCBI
Do I need imaging?
Most cases can start treatment without scans. X-rays may be used to screen for bone shape and joint changes; ultrasound or MRI are considered if symptoms persist beyond about 6 weeks of appropriate care or if another diagnosis is suspected. NCBI
Treatment:
Conservative care is first-line for the first 3–6 months when there’s no full-thickness tear or other structural red flags.
Core components are:
- Targeted exercise therapy: Strengthen the rotator cuff (especially supraspinatus/infraspinatus) and retrain scapular stabilisers (trapezius, serratus anterior) to correct dyskinesis and reduce superior humeral translation. NCBI
- Load management & education: Modify overhead workloads and aggravating positions while keeping general activity levels up. NCBI
- Short-term analgesia/anti-inflammatories (as appropriate) and subacromial injections for persistent inflammatory pain; ultrasound guidance may improve symptom relief compared with landmark-only techniques. NCBI
Surgery:
Surgery is not first choice for typical impingement without clear structural pathology. It may be considered after a well-supervised rehab trial fails and imaging confirms contributory anatomy or associated pathology (e.g., significant rotator-cuff tear). NCBI
Possible complications if untreated
Persistent symptoms can lead to secondary issues such as rotator-cuff tendinopathy or tears, biceps tendinopathy, and adhesive capsulitis (“frozen shoulder”). Early, guided rehab helps reduce these risks. NCBI
Prevention & self-care tips
- Gradually build overhead training loads; avoid sudden spikes.
- Optimise posture and workstation setup; vary tasks to limit repeated overhead time.
- Keep the shoulder blade “active” during lifts (think: ribs down, shoulder blade up-and-out), and maintain thoracic mobility.
- Continue your home exercise plan even after symptoms settle to maintain scapular control and cuff endurance. NCBI
When to seek help
- Night pain that doesn’t improve
- Pain or weakness persisting beyond a few weeks
- Traumatic onset, a feeling of instability, or marked loss of strength
Overall
- Shoulder impingement is a syndrome known as a cluster of symptoms and contributing factors, not just “bone rubbing on tendon.”
- Most people improve with a structured physiotherapy program that restores rotator-cuff strength and scapular mechanics, supported by sensible load modification and short-term pain control.
- Imaging and injections are used selectively; surgery is reserved for specific cases or failed rehab.
References:
Creech JA, Silver S. Shoulder Impingement Syndrome. StatPearls (NCBI Bookshelf). Last updated April 17, 2023